
There is increasingly clear evidence that older people are more likely to die from Covid-19 than are younger people: on 17th February, the China CDC weekly report showed that among the cases known in China by then, the ≥80 age group had the highest case fatality rate at 14.8% (with the 70-79 age group being 8% and the 60-69% age group being 3.6%); and in early April, the WHO Regional Director for Europe highlighted that over 95% of Covid-19 deaths occurred in those over 60, with more than 50% in those aged 80 years or older. In the UK, the Office for National Statistics (ONS) reported in mid-April that mortality from Covid-19 increased consistently with age, with only about 13% of deaths being of people under 65. Significantly, though it noted that men had a death rate double that of women; more recent ONS reports have also shown that (when taking into account age) Black men and women were more than four times as likely to die from Covid-19 then were those of White ethnicity, and that such differences in mortality were partly a result of socio-economic disadvantage. These data are stark, and are as yet still not fully explained. As people grow older, they generally have greater comorbidities, and it may be the impact that Covid-19 has on these other health problems that is more significant than age itself.
However, this is an important reminder that Covid-19 is primarily an old-people’s disease. It is striking to recall that in 1951 life expectancy at birth in England and Wales was only 66.4 for men and 71.5 for women; in 1901 the figures were 48.5 and 52.4 respectively (ONS, 2015). Put simply, people born 70 years ago were not expected to live to the age at which most people are now dying from Covid-19. This has important ramifications, and raises very difficult questions. Have people, perhaps, become over expectant about longevity? Will Covid-19 temper our aspirations to live for ever? Will it be a check on the ambitions of companies such as Novartis, Alphabet and Illumina to extend life well beyond 100 years (CNBC, 2019)? Is the main problem of Covid-19 that most people living in the richer countires of the world have become too cosy in their expectations of living to a ripe old age?
Implications for Europe and north America: too many old people
Thought experiments can be a helpful means of highlighting challenging issues. Suppose, for example, that there had been no lockdowns in Europe and North America. It seems very likely that substantial numbers of elderly people would have died already (see projections by epidemiologists at Imperial College which suggested that without mitigation strategies Covid-19 would have resulted in 40 milllion deaths globally in 2020). If a vaccine or cure is not found, then it still seems likely that large numbers of elderly people will indeed die in Europe at an age well short of what they and their families have grown accustomed to expecting.
However, think of the impact that this will have on the economy and health services. Once large numbers of elderly people have died, national pension bills will fall, the burden on health services will be reduced, the percentage of people within the economically productive age range will increase, and the economic vitality of their countries will be revitalised. If Covid-19 (or its successors) become an everyday part of life, the economic “burden” of older people will be dramatically reduced. It is scarcely surprising that rumours circulated about the intentions of UK government policy in early- to mid-March. As Martin Shaw noted at the time, it had been credibly reported that the “Government’s strategy was ‘herd immunity, protect the economy and if that means that some pensioners die, too bad’; or as summed up even more succinctly by a senior Tory, ‘Herd immunity and let the old people die’”. Whilst the government strenuosly denied this, there is a realistic logic to the idea that letting large numbers of old people die would have clear economic benefits, and would avoid the very considerable costs that are accruing as a result of economic shutdown.
I should stress that this is definitely not a scenario that I would want to encourage or endorse, but in the early part of May, the balance of popular opinion (or the influence of the business community and mainstream media in the UK) does seem to be swinging towards a view that the costs of lockdown are too high to continue to protect the elderly, especially in those countries where there have already been very high death rates (as in Belgium, the UK, France, Italy, Spain and the USA). Yet, the 20th and latest Imperial College Covid-19 report concludes for Italy that “even a 20% return to pre-lockdown mobility could lead to a resurgence in the number of deaths far greater than experienced in the current wave in several regions”.
Implications for Africa and South Asia: youthful countries
The real purpose of this reflection, though, is to consider the implications of the above arguments for some of the economically poorest countries in the world. Data about Covid-19 infections and deaths in Africa and Asia are likely to be even less reliable than they are in Europe, and the countries in these continents are in any case much earlier in their encounters with Covid-19 than are those of Europe. Recent reports, for example, suggest that the real number of deaths related to Covid-19 may be many times the number that are currently reported (see The Guardian‘s recent report on Somalia). Nevertheless, we do have relatively accurate data about the demographic structures of most countries in the world. The chart below therefore shows the relationships between current density of Covid-19 deaths and the percentage of population aged ≥65 for a sample of countries.[i]
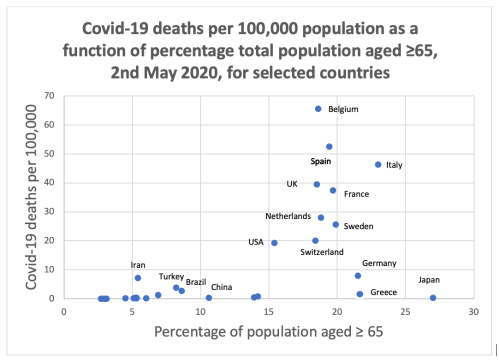
This graph is striking, but difficut to interpret (and can be misleading), mainly because most countries in Africa and Latin America are only at an early stage in their Covid-19 outbreaks. We simply do not know how many deaths they are likely to witness, and few models have yet been published that predict the likely outcomes. However, with the very notable exceptions of Japan, Greece and Germany, it re-emphasises that high percentages of Covid-19 deaths are mainly found in those countries that have more than 15% of their populations aged ≥65. Even Brazil, where the death rate is currently growing rapidly, is still nowhere near at the level of mortality that has occurred in Europe and the USA. The quite remarkable achievement of Greece, with only 147 deaths by 7th May, is also highly noteworthy because despite a fragile health service and an elderly population it has managed to achieve something that most other European countries have been unable to do. Most commentators suggest that this is mainly because it imposed a dramatic lockdown even before the first deaths were recorded.
Most countries of the world have intiated lockdowns, and these are having particularly significant impacts on the poorest and most marginalised who can least afford it. An obvious question therefore arises: if Covid-19 mainly affects the elderly, should countries with young populations (such as most of those of Africa, Asia and Latin America) follow the “older” countries in imposing strict lockdowns that will have damaging effects on their economies and the livelihoods of those who can least afford it? Put another way, are the mitigating actions of European and North American countries, where more than 15% of their populations are ≥65, relevant to economically poorer countries with less than 10% of their populations in this age group?
It is far from easy to answer this. Perhaps the very small numbers of people reportedly dying in Africa at present is only because the coronavirus has not yet gained a grip, and any loosening of the mitigating measures would unleash the pandemic at a scale similar to that seen in Europe. The WHO, for example, has warned that the Covid-19 pandemic might kill as many as 190,000 people in Africa in the year ahead (Al Jazeera, 8th May), with many more dying subsequently. This may well be true, but there is at least a chance that the youthful populations of Africa will be better able to deal with Covid-19 than have done the older populations of Europe. It must, though, be emphasised that many younger people who are infected with Covid-19 do indeed have serious illnesses, and some die. We also do not yet know the long-term health impacts of this coronavirus. Moreover, the evidence that socially disadvantaged people are also more likely to die than their more affluent neighbours further suggests that the poorest and most marginalised in these countries may well have higher death rates.
As I have illustrated elsewhere, there is some (but by no means conclusive) evidence that environmental factors may also play a role in limiting the spread of Covid-19. If the environments of Africa and South Asia are indeed not particularly conducive to the spread of Covid-19, then their youthful populations might not need to endure the very tight lockdowns imposed in many European countries. That having been said, the rapidly increasing number of infections and deaths in Brazil (with 121,600 cases and 8,022 deaths as of 7th May), which has physical environments and climates similar to many parts of western and southern Africa, does not bode well for the future spread of Covid-19 in Africa.
Conclusions
In conclusion, there remains much that is unknown about how Covid-19 spreads and who it affects most damagingly. The evidence from Japan, Greece and Germany shows that even when countries do have a high percentage of elderly people, it is still possible to contain and limit the spread of Covid-19, thereby preventing very large numbers of deaths. The abject failures of governments in countries such as the UK and Belgium to manage the pandemic and save lives likewise indicate how not to respond to the pandemic. The governments of African and South Asian countries, with their youthful populations who appear less likely to suffer severe symptoms, may well therefore have an advantage over their European counterparts. If they can draw lessons about what has worked and what has failed, then they are also in a good position to bounce back swiftly from the economic harm caused by economic and social lockdowns.
[i] The selected countries included the ten most populous countries in the world (in descending order of total population, China, India, USA, Indonesia, Pakistan, Brazil, Nigeria, Bangladesh, Russia, Mexico), a selection of European countries with mixed trajectories (listed alphabetically, Belgium, France, Germany, Greece, Italy, the Netherlands, Spain, Sweden, Switzerland), and a diverse sample of African (alphabetically, DRC, Egypt, Kenya, Rwanda, South Africa, Tanzania), and other (alphabetically, Iran, Japan, South Korea, Turkey) countries.


Great piece Tim, plenty to consider and debate there…..
How is the replaced hip performing some years on ?
Regards,
Paul Hutchings
Thanks Paul. Still doing well – although frustrating that I should not/cannot really use it for running. So, towards the end of last year I got a fitness bike for use at home – tough, but keeps me doing some exercise, and helped me reduce weight. This has become so very much more valuable in lockdown, as we face all the unknowns of Covid-19. Keep well yourself!
Good to hear that its performing well.
Like you, I decided not to run again in order to make the hip last longer. I took up swimming and not being lucky enough to own one at home, haven’t been swimming since lockdown.
Cycling has been good release though.
Hip functioning lovely & pain free however, knee is starting to become a little more painful. I am far more concerned about having the knee done than I ever was the hip so going to wait until I retire in 2 years time. Stay safe Tim.
Pingback: A differentiated, responsibilities-based approach to living with the Covid-19 pandemic | Tim Unwin's Blog